Your Questions
Your Questions
Q: Dr. Eppley, is there a safe surgical method to correct frontal bossing of the forehead? I have read online on some medical websites that there is no surgical fix but on Dr. Eppley’s website I noticed there were a few photos. My son is 21 and is experiencing some hair loss already in his hairline which exposes his forehead more and we are looking at hair transplant surgery which may help, however I wondered if there was a surgical repair that could safely be done and what that may entail. Thank you for any information you can provide.
A:Bony forehead reduction (frontal bossing reduction)can be performed in anyone. The question is not whether the forehead bossing can be reduced but by how much and whether that amount would be satisfactory to the patient. That I can not tell you without seeing pictures of the forehead in profile and ultimately a side x-ray of the forehead to measure the bone thickness of the outer cortical table. Like any type of skull reductions there are limits as to how much bone can be safely removed. So whatever amount can be removed, even if it falls short of the patient’s ideal goal, is the result a patient has to accept. Thus it becomes important to have a good idea before surgery as to what can be achieved.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had jaw angle implants two months ago and the left side has been swollen ever since. I now seem to have a parotid gland leak on the left side that stems from the frontal edge of the jaw angle implant that may or may not also be an infection. I am fairly sure it is a parotid leak because it has swelled up twice painfully upon eating spicy food. The first time the swelling lasted almost two months, and this time happened again just a day ago. If I remove the implant on the left side, will this be resolved? Will I need a drain, etc.?
A:I have never seen a parotid gland leak from jaw angle implant surgery nor can I imagine how that would be possible since the mandibular vestibule and/or ascending ramus is positioned much lower than the parotid duct. I can only assume that the chronic swelling on the left side causes some partial obstruction of the parotid gland when highly simulated. This is ductal obstruction not a gland leak. It would be anticipated that that thighs will remove when the implant and its associated swelling resolves.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’m a young male. My head is convex at the out direction near my ears. I’ve always been self conscious about the width of my head. If you injected Botox into the muscle would it affect the temple muscle on the side and shrink that. I have seen pictures of people getting the injection done near the eyes for crows feet with deep impressions on their face after associated with temporal wasting.
These are photos of what I’m looking for before and after. I’d like to shrink it 5-7mm. Thats what this photo shows. In my opinion its a big difference.
I’m not big on plastic surgery. this is more of a self conscious thing. I’m not interested in excision of the muscle. Is this something you’ve done before with botox and had success before. Do I need an X-ray before determining if its possible. And would you be able to promise something like this doesn’t happen. This person got injections near the eyebrow for crows feet and the temporal muscle shrank that it gave this indentation. Thanks, hope to hear from you soon.
A: Thank you for your inquiry and sending your desired result. That type of side of the head width reduction is only achievable by removal of the posterior temporal muscle which is 5mm to 7mms thick in most Caucasians. Botox injections will not create that amount of shrinkage no matter what dosage is used as the temporal muscle is bog and thick. And even if it did, it will last less than three months after the injections. Botox does not cause permanent atrophy of the masticatory muscles. I have never seen anterior temporal wasting with crow’s feet Botox injections or any form of posterior temporal muscle reduction surgery.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, my question to you is if you could diagnose my head shape. I am having issues with understanding what the condition is it’s either deformational plagiocephaly or lamboid craniosynostosis. They look very similar but I don’t know which one it is. It could be possibly be something else but I don’t know so if you could help me out with this issue I would be truly grateful.
A: Only a 3D CT scan can separate those potential diagnoses for the flat back of your head. It will show whether the lambdoid sutures are open or closed which will provide the diagnosis. Statistically speaking it is far more likely it is deformational plagiocephaly than lambdoid craniosynostosis which is much more uncommon and would present with more severe flattening.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’ve been dealing with neck issues for my entire life. I do not yet know what is exactly wrong. I don’t think I have a webbed neck but a slightly thicker one I know I do have that… if it is caused by my uneven collar bones from once being broken I’m unsure, I just want it treated. It gives me bad self esteem issues, to the point were I do not wear my hair up around others. I can’t work efficiently and honestly I would just like to fix this or improve upon this issue so my life can be a little less hindered! I just want to be at the point where if I am sweating I can put my hair up and not have people comment on my appearance. 🙂
A: Thank you for your inquiry and sending your picture. You do have a webbed neck deformity which has a fairly classic appearance in non-syndromic patients which can be treated by a webbed neck surgery. Your right clavicle is also more prominent than the left, presumably due to the previous fracture. The only way to reduce its prominence is by a shave technique.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Is there a age limit for reducing sagittal raised bump at the top back end of the head? Is it dangerous? How long does a procedure like this take? Thanks
A:In answer to you posterior sagittal crest skull reduction questions:
1) There is no age limit. Anyone under age 18 needs parental consent.
2) It is a one hour procedure.
3) It is perfectly safe surgery.
Dr. Barry Eppley
Indianapolis Indiana
Q: Dr. Eppley, I had a bilateral orchiectomy March 2018 when large Torosa saline filled Implants where placed through the openings on each side of my scrotum. Unfortunately things would not heal and kept pulling the sutures pull apart. I had to have them removed last year. This December I had medium ones installed using the Inguinal method and all has healed well. I am not happy with the size however and would like something larger than the Torosa large saline filled implants. The saline filled implants are hard and you can deal the attachment tabs and fill ports. What options do you offer…?
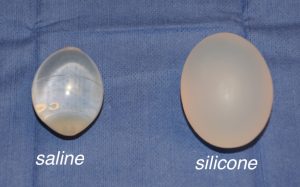 A: I never use saline testicle implants as they are usually too small and always are too firm and don’t feel like natural testicles. (which of course are not a bag filled with water under high pressure) I use ultrasoft solid testicle implants that are available in standard sizes up to 6cms and larger with custom designs. I use a midline scrotal raphe incision which provides more direct access to the implantation site and heals in a virtual scarless manner.
A: I never use saline testicle implants as they are usually too small and always are too firm and don’t feel like natural testicles. (which of course are not a bag filled with water under high pressure) I use ultrasoft solid testicle implants that are available in standard sizes up to 6cms and larger with custom designs. I use a midline scrotal raphe incision which provides more direct access to the implantation site and heals in a virtual scarless manner.
Dr. Barry Eppley
Indianapolis Indiana
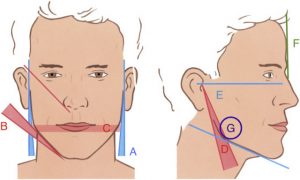 Q: Dr. Eppley, I have a question for you pertaining to custom jaw implant design, particularly in regards to the vertical length of the ramus. Based on my research, it seems an optimum aesthetic result in men is one where the jaw angles are in line with the labial commissure of the mouth (and not below the lower lip) when the head is looking straight at the camera. How would you incorporate this in an implant design to achieve this effect given that the teeth are not always a good indication (i.e., that depends on the face’s forward growth)? I very much look forward to your opinion on this.
Q: Dr. Eppley, I have a question for you pertaining to custom jaw implant design, particularly in regards to the vertical length of the ramus. Based on my research, it seems an optimum aesthetic result in men is one where the jaw angles are in line with the labial commissure of the mouth (and not below the lower lip) when the head is looking straight at the camera. How would you incorporate this in an implant design to achieve this effect given that the teeth are not always a good indication (i.e., that depends on the face’s forward growth)? I very much look forward to your opinion on this.
A: When it comes to the best jaw angle shape and placement in any patient this must be determined in an individual basis. I am well aware of the research to which you speak and, while this may be a general guideline, it is theoretical based on averages and most certainly does not apply to every male jawline augmentation patient in my experience. This is where the role of computer imaging is essential in preoperative planning to find the jaw angle location that looks best to the patient.
Dr. Barry Eppley
Indianapolis Indiana
Q: Dr. Eppley, Hello. A question…can PMMA BONE CEMENT be used for face augmentation as in: infraorbital, zygoma, maxilla and malar regions. And does it work permanently or it shrink over time.
Best regards
A:The problem with PMMA bone cement is that it is impossible to place it and get it to have the desired shape and symmetry between the two sides of the face. It is a moldable putty which has to be intraoperatively shaped and then allowed to cure and set. This concept works well in a wide open implantation site like the skull but is much more technically challenging in the very limited incisional accesses used in the face. For very small facial augmentations this might work but not for most of the type of facial augmentations that most men seek.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I believe that my mouth is too small for my face and I seek a way of rectifying it. Lateral commissuroplasty seems to be the best approach to solve this issue however I’m seriously concerned about the potential scarring that may arise because of this. From my research the area around the corners of the mouth tend to scar easily . If this is the case can the scarring be diminished or even eliminated with scar revision surgery?
 A: Thank you for your inquiry from which your two assumptions are correct; 1) effective mouth widening can only be done surgically by a uniquely designed lateral commissuroplasty design, and 2) the corners of the mouth are uniquely sensitive to scarring. In order to favorably combine the two concepts, 1) get an effective result and 2) not result in undue scarring, I employ two mouth widening strategies. First the amount of surgical mouth widening should be limited to no more than 7mms per side. Secondly it is reasonable to assume that the risk of needing a scar revision for one side (of which there seems to nearly always be a good side and a ‘bad’ side in the patient who may have a scar concern) is 50%. Scar revisions surgery is about diminishing its appearance, there is no such outcome as complete scar elimination.
A: Thank you for your inquiry from which your two assumptions are correct; 1) effective mouth widening can only be done surgically by a uniquely designed lateral commissuroplasty design, and 2) the corners of the mouth are uniquely sensitive to scarring. In order to favorably combine the two concepts, 1) get an effective result and 2) not result in undue scarring, I employ two mouth widening strategies. First the amount of surgical mouth widening should be limited to no more than 7mms per side. Secondly it is reasonable to assume that the risk of needing a scar revision for one side (of which there seems to nearly always be a good side and a ‘bad’ side in the patient who may have a scar concern) is 50%. Scar revisions surgery is about diminishing its appearance, there is no such outcome as complete scar elimination.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’m almost exactly 6 months post op from my genioplasty last October. I’m not really experiencing any numbness/pain or complications, which is great, and I’m happy with my results of my surgery overall. The only thing is that the projection of my chin is a little bit less than what I had hoped for, and I still feel like my chin appears slightly weak from profile
Here are a few pictures so you can see what I mean. The first one is a recent picture, the second is the imaging we did for the genioplasty and the third is pre-genioplasty.
I wanted to know if you think it would be worthwhile to consider a genioplasty revision to advance the chin more? Or if it’s a better idea to utilize a more minor treatment like chin filler. Curious to see what you think- I am interested in getting slightly more projection but don’t want to “play with fire” if I already have a good result and revision would be risky.
Thanks for everything!
A: Good to hear from you and thank you for sending your long-term results. I think the question is not whether it is a choice between a secondary sliding genioplasty or injectable filler, as you are too young to continue to have filler treatments for decades into the future. I think the better question is whether to have a secondary sliding genioplasty or place a small chin implant in front of the existing position of the chin bone. It looks like the additional change would be about 3mms more horizontal projection.. I can make an argument for either approach. A very small chin implant is far simpler for you with quicker recovery….but it is an implant. Conversely you have had a uncomplicated recovery from the sliding genioplasty and the same identical bone cut would be used….so one would expect a repeat outcome/recovery experience in that regard. In other words it is not more riskier the second time.
Dr. Barry Eppley
Indianapolis Indiana
Q: Dr. Eppley, I am interested in hip silicone augmentation as I have no fat and my hips are kind of narrow I would say. What is the largest hip implant you have/can make for me and what is the price? I want big hips like Kylie Jenner. Do you do silicone injections maybe? Thank you
A: Thank you for your inquiry. I do not do silicone injections as they are fraught with potential problems and silicone oil is not an FDA-approved material for any form of body augmentation. I also do not do ‘big’ hip implants as that is just a complication waiting to happen. Hip implants are placed on top the muscle fascia and as a result have a higher incidence of complications than other body implants. Thus it is best to have only moderately sized implant to lower the risk of potential problems. A good concept to remember in that regard is ‘it is better to have 50% of the result you want with no complications than 100% of the result you want with complications’.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I want a Breast Fat Transfer with PRP procedure. I had 2 children 4 years apart. I breastfeed each child for 1 year. I lost a lot of breast tissue while breastfeeding. I want to regain the fullness and also firmness I once had before breastfeeding.
A: Thank you for sending your picture. Unfortunately you are not a good candidate for breast augmentation by fat transfer for two specific reasons. First you lack adequate fat to harvest for the procedure. Using the 50% rule in fat injection augmentation, 50% of the aspirated volume removed by liposuction is lost by pre-injection concentration, then what is left is divided in half because there are two breasts to inject and then assume only 50% of the fat will survive. To put that into perspective let’s assume you could harvest 2,000ccs from you (which is a big assumption), after concentration 1,000ccs is left in which 500cc is injected into each breast of which 250ccs will survive. (the equivalent of a very small breast implant or the same volume as a glass of water) Secondly, although your breasts are covered and does not reveal how much loose breast tissue you have or whether you have any sag…which I suspect you might), a 250cc volume addition is not going to adequately replace a lot of breast tissue loss and is not going to fill them up or make hour breasts firm.
Breast augmentation by fat injection works best in the patient who only wants about a 1/2 cup size volume fill and has good breast skin with little to no sag. Your current breast shape and goals can really only be met by conventional implant and/or lifting procedures in my opinion.
Dr. Barry Eppley
Indianapolis Indiana
Q: Dr. Eppley, You recently replied to one of my questions on Real Self website. I was inquiring about the feasibility of correcting my lower face asymmetry, particularly my chin, which as you can see is deviated left, off-center, and slightly recessed. You said a custom chin implant would yield better results than a sliding genioplasty. Out of curiosity, what is the price range for a custom chin implant? Will the custom chin implant improve the contour and definition of my right jawline as well? What is the price range for a sliding genioplasty? And will a sliding genioplasty improve the contour and definition of my right jawline? I am very seriously considering getting a procedure done with you because of your reviews and before/after photos so any basic information you can provide regarding my questions will be helpful before I schedule an official consultation.
A: In chin asymmetry in which the patient also desires horizontal augmentation there are two approaches that can be used as you have mentioned, custom chin implant and a sliding genioplasty. If one is just looking at the best result the custom chin implant is superior because the preoperative design can make all of the dimensional changes in a controlled preoperative fashion with an implant that exactly fits the patient’s anatomy. While a sliding genioplasty can also be done, and is the historic procedure for such chin asymmetries/augmentation, it relies on the surgeon’s eye to align the chin and creates bone cuts through the inferior border of the lower jaw on both sides that will be irregular afterwards. While one can place allogeneic bone paste into these genioplasty bone irregularities that is not an assurance they will be perfectly smooth and even.
The only reason to choose a sliding genioplasty over a custom implant, which are perfectly valid, is cost or if one is opposed to the use of implant. But based on aesthetic outcome alone the custom chin implant design is by far the superior approach.
In a chin that is deviated and short almost assuredly the jawline on that side as well is probably underdeveloped. Only a custom implant design can correct that as well, a sliding genioplasty can not.
Dr. Barry Eppley
Indianapolis Indiana
Q: Dr. Eppley, sorry for showing images again but I was looking and realized the right side of my face is the only part that bothers me and I’m wondering if theres just a small implant that can make it the same as my left side to correct my jaw angle asymmetry.. I can see that on my good side the angle is a little closer to my ear, a little longer, and a little thicker. Also you might not see it but the area beside my ear is also a lot more hollow than my other side. (Can easily feel it) not sure if the bone in the area isn’t as thick or if the muscle is weaker.
A: While one could use just a ‘small’ implant for the right side, there are always problems with standard implants for asymmetry problems. And the problem is the smaller the problem is the harder it is to get it symmetric. Often you just create a different type of asymmetry. But if one was to use a standard implant for just one side, you have better have a 3D CT scan to take measurements for how the implant should shaped. Or even use an engineer to establish the dimensions of what would be the exact dimensions that the implant needs to be.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am a middle-aged male. When I was a baby I had craniosynostosis for which I had surgery. I have a flat spot or dent on the crown of my head so I was reaching out to see if you performs procedures to fix an issue like this.
A: Thank you for your inquiry. Many patients with cranial vault surgery as infants do have residual skull contours (partial defects) and even full-thickness defects. Since you probably have a coronal scalp incision to some extent that could be used as access to fill in the defect. Whether that is best done with bone cements or a custom skull implant would depend on the location, size and whether the defect is partial or full thickness. A 3D Skull CT scan is needed to help guide the cranioplasty technique used.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I was talking to you about chin shortening a while back but I gave up on the idea. The more I look I feel like a custom jaw implant would be better. In the pic I drew is pretty much how I’d like it. Keeping the angle just making it straight and pushing the corner back some. Only thing is I don’t really want it to change the front of my face so its like vertical length implants thats on your website. (Dont want the wide square look) Let me know what you think.
A: It appears you have figured out that the real problem is not that the front of the lower jaw is too long but that the back of the jaw is too high. That would create a more proportionate and balanced face. The only caveat I would say is that you may want to bring the back down a bit but you don’t want to make the corner of the jaw angle go back. That is a recipe for creating the problem known as ‘implant reveal’ often confused with masseteric muscle dehiscence but it appears the same. The anatomy of that muscle is that its length is tied to were it naturally attaches to the bone. Thus as the jaw angle comes down a bit it needs to largely keep that same more rounded shape…otherwise the implant will stick out from behind the muscle like a square lump.
It is a common misconception that a square jaw look comes from a square bony shape…which is incorrect. Even the most square male jaw angle you have ever seen (Non-Asian) the jaw angle bone shape is not square.
Also every vertical lengthening jaw angle implant will make the face from the front change shape…you can’t avoid that. It can only be mitigated somewhat by not having too much width in the vertical drop down.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have a general quick question.
Can a skull reshaping surgery of the back , top and sides increase the skull size and circumference?
A: You are referring to a custom skull implant that covers the top, back and sides of the skull. Such an implant can augment all of these areas within the limits of how much the overlying scalp can stretch to accommodate it. In most of such cases of skull augmentation it is usually necessary to do a first stage scalp expansion to get the type of head augmentation result most people seek who would ask this question.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have a sagittal ridge that extends to my forehead. I have a couple of questions:
– general cost
– is financing available
– i live on long island, how many visits would be required to indiana
– how long would the proceedure last
– how long would i be out of work
A: In answer to your sagittal ridge reduction questions:
1) Only one visit is needed for the surgery.
2) The procedure is completed in 90 minutes.
3) I don’t know what type of work you do but it should only be one week at most.
4) My assistant Camille will pass along the cost of the surgery to you.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I was hoping you could tell me whether or not my lip reduction goals are realistic. Would it be possible to remove enough tissue from both lips that they would “fit inside” the template shown in the attached photo rather than go outside the lines? If this can be achieved, would it be done by removing tissue from the dry vermillion where it meets the skin or the wet vermillion where the scar is hidden inside the mouth?
Thanks in advance
A: As a general rule in my experience you can effectively reduce the size of the central upper and lower lips by about 1/3.The tissue removal has to be at the wet-dry vermilion junction with the linear removal of tissue being the dry vermilion. This rolls back the exposed dry vermilion. You don’t take wet mucosa as that tissue is very stretchable and it will accomplish to little to no actual reduction as the wet mucosa then just gets pulled up into the wet-dry line closure. You also never try to do a lip reduction by removing dry vermilion at the vermilion-cutaneous line as the skin is fixed and will not make the lip pull in or get smaller.
The imaged results you have shown are within the range of what one cold probably expect. In short, it is not an unrealistic goal.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I found your web site by chance while I was searching for medical treatment regarding Plagiocephaly, I was just thinking to resolve the problem once for all as it is disturbs me all the time, so I wanted to pose some questions:
How much it would cost roughly, more or less, the surgery of occipital surgery for the flathead for not US citizens?
How much time it is needed for treatment? (surgery plus recovery)?
Is it safe procedure or there might be some collateral damage?
thanks in advance!
A: Thank you for your inquiry. In answer to your plagiocephaly questions:
1) The most common treatment for lagiocephaly is a custom occipital implant for the flat side of the back of the head. I assume this is your concern as well.
2) Such custom occipital skull implant surgery takes 90 minutes to perform. The implant is preoperatively designed from a 3D CT scat of the patient six weeks before their surgery. Recovery is fairly short in the 10 day to 2 week period until one is back to all normal activities.
3) My assistant Camille will pass along the cost of the surgery to you.
4) This is a very safe procedure as the implant sits on top of the skull bone under the scalp.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I got married in September 2018 and now have a baby boy. I will attach pictures. I quit breastfeeding in February, and my boobs feel extremely empty so I am considering breast implants. However, we want to have one more baby so what are your thoughts on waiting until the second one is over? I had to have a C-section because he was breech and they said I will have to have another one. Not sure this even matters, but wanted to let you know. We plan on starting to try this fall/winter and the last one happened right away so if I wait it would put me out a couple years. Hopefully you won’t retire on me if I wait 🙂 Anyways, wanted to see what your thoughts were. Also, could you provide me with a price range for this type of procedure? I wouldn’t want to go much larger than what I already had, which was 32C, so probably a fuller C, smaller D. I hope all is well with the family and you! Look forward to hearing from you! Thanks in advance for your time and guidance!
A: Good to hear from you and congratulations on your beautiful baby boy. Because pregnancy creates breast changes, as you now know well, if you know you are going to have another child it is always better to wait so the surgical result will be stable. Other than large amounts of weight loss, pregnancy creates the greatest havoc on the breasts. After pregnancies, unless one gains a whole lot of weight and then loses it (which will not happen to you), there isn’t much to really change the breasts so one’s investment is better protected long term.
Stay healthy and well and I’ll see you in a few years!
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had an endoscopic brow lift seven months ago and my eyebrows are too high and my forehead is now too big is it possible to reverse it without a scar on my hair line as my hair is very fine. Thank you.
A: Thank you for your inquiry. Although I don’t know exactly what you looked like before or after your brow lift surgery, the conceptual basis of your question can be addressed. An endoscopic browlift works by the principle of an epicranial shift….unlike all other forms of browlifting. While the entry incisions are small what is done underneath the entire forehead, brows and the scalp behind it is to release all the tissue attachments from the bone. The forehead and scalp is then shifted backward and secured where it heals back down to the bone in the new elevated eyebrow position. With that becomes an expected, although often not appreciated, elevation of the hairline and forehead lengthening. (which is minor in some patients and more significant in others) The key concept here is that the browlift works, not by removing tissues, but by changing their position on the skull. Thus there is no tissue loss which is really important when thinking about how to reverse it.
As a result of no tissue loss, in theory, an endoscopic browlift is reversible. If the epicramial shift process is reversed (full forehead and scalp mobilization) and fixation done in the opposite direction through the same incisions it should at least be partially reversed. (which I imagine is the goal rather than full reversal since there is a reason you had the procedure done initially)
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in your skull reshaping procedures. I am a young male, and the shape of the upper third of my skull can be described as narrow. Specifically, my frontal bone is narrow. This includes my supraorbital rim, my forehead, and the very top of the frontal bone which forms the top of the skull.
So I want to widen this area. I envision a customised implant broadening the supraorbital and the very top of the lateral orbital rim; through to forehead widening; and finally a widening of the top of the skull. In order of priority; the most important aspect for me is the supraorbital rim, because this frames the eye area.
The second aspect of my frontal bone is that is quite rounded and feminine. What I mean by this is that the lateral areas of the frontal bone sit too far back relative to the centre of the frontal bone. In other words, the sides of the frontal bone ‘fall away’ too much, which is a feminine aesthetic. Masculine frontal bones have a much smaller discrepancy between the anterior position of the centre of the frontal bone, and the anterior position of the lateral portion of the frontal bone.
I know that this procedure is theoretically possible, but I anticipate several issues, which I will now enumerate:
1) How does one widen the frontal bone beyond the anterior temporal lines without creating problematic aesthetic issues? What needs to be done to accomplish this, without it looking unnatural? Surely the position of the temporalis muscle is a limiting factor here?
2) How does one compensate for the concavity that will be created in the temporal area? If the brow and forehead are widened, with the temporal area remaining the same; there will be a visible concavity in this area which may look unnatural
3) If a combined temporal-frontal bone implant is used, how does one maintain the natural delineation between these two areas? Blending the two regions into one monolithic region would be an aesthetic limiting factor for me, because the majority of people have some visible distinction.
4) I believe in an aesthetic that preserves the harmony between the width of the various facial structures. Observing many aesthetic faces, there is usually no issue if the zygomatic bone is wider than the mandible or maxilla. However, the relative widths of the frontal bone and the zygomatic bone is usually a significant factor. In my opinion, that is because the two bones are directly connected at the lateral orbital rim. Widening just the frontal bone here would create disharmony between these two bones. So I am interested in your opinion regarding concomitant widening of the entire lateral orbital rim and the zygomatic bone (chiefly the zygomatic arch and the part of the zygoma just beneath the eye). In your experience, would this be aesthetically feasible, and what issues might you anticipate with this?
I do apologise if I have taken up your time with these questions. Understanding these issues in detail is crucial for me to consider getting this custom skull implant, and I hope you can help me out here.
Thanks.
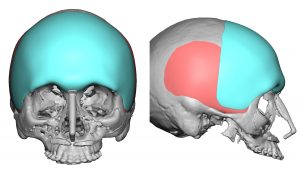
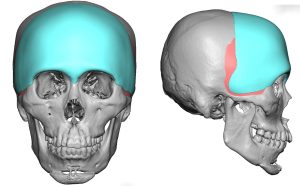 A: Thank you for your inquiry and your very articulate and intellectual description of your aesthetic head shape concerns, objectives and the aesthetic challenges that come with trying to rectify them all in a proportionate and harmonious manner. I will answer your questions in detail but have attached a few prior patient custom skull implant designs in the spirit of ‘a picture is worth a thousand words’ that have addressed similar patient concerns.
A: Thank you for your inquiry and your very articulate and intellectual description of your aesthetic head shape concerns, objectives and the aesthetic challenges that come with trying to rectify them all in a proportionate and harmonious manner. I will answer your questions in detail but have attached a few prior patient custom skull implant designs in the spirit of ‘a picture is worth a thousand words’ that have addressed similar patient concerns.
1) Any implant design that needs to go past the bony temporal line will sit on top of the temporalis fascia/muscle.
2) Depending upon how much the implant design crosses the temporal and how much forehead width and frontal augmentation is needed, the implant design may have to cover the anterior temporal region to prevent creating unaesthetic temporal hollowing.
3) In men you design as part of the implant a temporal line of transition between the forehead and the temporal area. (subtle raised ridge) In women this is not necessary.
4) While you can extend an implant design down along the lateral orbital rim and cover the temporal area as well, you can not cross onto the zygomatic arch. There are rigid attachments of the periosteum of the zygomatic arch over which courses the frontal branch of the facial nerve. Elevating this periosteum off of the zygomatic arch will injure that nerve and cause permanent paralysis of the forehead muscle elevators which are responsible for eyebrow movement. As a result any augmentation of the zygomatic arch must be done with a separate implant from a different point of access.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, My left hemimandible has a much better angle and definition than my right hemimandible which is not as pronounced and is vertically higher if that makes sense. Attached is also a childhood photo (because at first I was thinking this is a mild version of hemifacial microsomia, however when looking at my childhood photo I appear to be relatively symmetrical insofar as my jaw/cheek/ears are concerned so I am not so sure this is the diagnosis. The asymmetry didn’t manifest or become very apparent until my teenage years when I had four years of braces while going through puberty). When I was 16 and my braces came off I sought out a maxillofacial/plastic surgeon who at that time advised I wait until I am older/have fully matured before seeking corrective surgery. I am currently 24 years old, ultimately happy with the way I look especially on the left side of my face, however my goal is just to make my right side as symmetrical to the left as possible.
A: Thank you for your inquiry and sending your pictures. The type of jaw asymmetry you have is the most common and presents just as you have by:
1) Usually only appearing after puberty
2) One jaw angle will be higher and less defined and the other lower and more defined.
3) The male preference is almost always for the lower more defined side of the jaw.
Such jaw asymmetries are evaluated by a 3D CT scan and treated by the design and placement of a custom implant to build up the higher asymmetric side.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am 21 years old and have scoliosis. My ribs stick out very far and aren’t even. I was thinking about rib removal but I wanted to know if you think it’s the right procedure for me. I am very insecure and have always wanted to have a normal torso.
A: Thank you for your inquiry and sending your picture. You have subcostal rib protrusion which is not rare and is very common in patients with scoliosis. The scoliosis usually makes ones one side stick out further than the other. But like any patient with anterior subcostal rib protrusion the question is not whether they can have rib removal surgery but whether the aesthetic tradeoff to do so is a worthy one. I am specifically referring to the fine line scar on each side which would lie right along the protrusion and be about 6 cms long on each side. I always ask this question to every patient because such a scar location is in a non-hidden location and you want to be sure that you don’t tradeoff one problem for another one you may dislike just as much. I am not saying it is a bad scar or is not a better tradeoff, it is simply the question that each patient has to answer for themselves as that answer determines the benefits of the procedure for any patient.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, is head reshaping surgery safe ? What are eventual complications ? And what’s the price of this intervention? And how many time takes the operation?
A: You would have to provide more information as to what your head shape concerns are so I can determine what is the procedure you need. There are over 25 different types of skull reshaping surgeries that I do.
But the one question I can answer for certain right now is that all skull reshaping or head reshaping procedures are safe or I wouldn’t be doing them. They are as safe as any other aesthetic face surgery. And of all areas on the body that undergo aesthetic changes skull reshaping procedures have the lowest incidence of complications and need for revision surgery.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I stumbled across a question someone asked that is the exact issue I’m having and have been trying to research a solution for. Someone asked “Can my Malar Fat Pads be removed by liposuction” as it was prominent on the persons cheekbones once they smiled, and not exactly a buccal fat issue. I’ve attached a screenshot of the Question/Answer for reference. This is exactly the question/issue I have so I appreciate your response. My follow up question is now what CAN be done as alternative solutions or have you performed any type of treatment to address this, as he acknowledged complete removal is likely not possible/effective but not to say that it couldn’t be addressed. I’ve been struggling with this for years and looked into Cheek Reduction surgeries performed in South Korea, but even this doesn’t appear to be what I’m looking for either as that seems to move volume in cheekbones from the high sides to the front of the face for a youthful appearance, which is the exact opposite of what I’m looking for despite the fact that a “cheekbone reduction” by the name alone sounds like what I want. I look much younger than I am due to this (not really why I dislike it, it’s more so that it becomes extremely exaggerated in photos to the point where I don’t look like myself in photos, almost looks like a ventriloquist doll). I’m looking for the fat only to be lessened and not the cheekbone itself to be moved, as suggested in the Korean surgeries. Also, I find that my smile gets stunted (and that part I’m not sure if that is a buccle fat issue. My dentist acknowledged that I have a small mouth which I feel is because of potential full cheeks. I find it similar to smile/full cheeks of Khloe Kardashian or Scarlett Johanson when they smile as opposed to the wide smile of say Cameron Diaz, if that makes sense). Look forward to hearing from you!
A: As stated in your posted answer of mine from an identical inquiry on the same topic, such malar fullness/fat ‘pad’ is not treatable by a surgical procedure. It is not a discrete fat pad like the buccal fat pad that can be excised and it is composed of fibrofatty tissue that is largely resistant to liposuction not to mention the buccal branches of the facial nerve which course through this area and thus risk injury.
The only alternative to try is non-surgical and that is energy-based reduction. One of the well known unintended and adverse effects of skin tightening devices is underlying soft tissue atrophy due to the consequences of heat on fat. While not intended this concept can be used for problematic facial fatty areas that are not amenable to surgery. We use it for such problems and in particular to help reduce undesired fat injection results. It usually takes multiple treatments to see its full effects but it is at least associated with no risks….it either works a little bit or it works a lot.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am have quite a few different questions about some surgery.
Is Jaw Angle Reduction something you do? I would like to reduce the squareness in my jaw and take the angle higher towards my ears rather than being horizontal across my face.
Are you able to surgically lower the eyebrows? Where would the scar be located for this if possible?
My cheekbones are quite wide and jut out horizontally below my eye, causing my face to look wide. Is there anything that could be done for this?
Final question, I know the answer is almost certainly a no.. but is there any way to reduce the width of the hip bones? Even just a little bit? I am Male with a BMI of 20.4 and my hip measurement is 39.5″.
Thank you so much in advance for taking the time to read my questions, I hope to hear from you soon.
A: Thank you for your inquiry. In answer to your fat and hip bone questions:
1) For your jaw angle reduction you are referring to two types of dimensional changes…reduction in squareness and possible elevation of the inferior border. By description that would indicate a jaw angle excision or amputation technique. Whether that would be the appropriate method for you requires a preoperative 3D CT scan to evaluate the anatomy. For many Non-Asian patients the jaw angles look lower than what they really are because of the flare of the outer cortex. Once the flare is reduced the angle instantly looks higher.
2) I know of no guaranteed way to lower the eyebrows short of a 1st stage forehead tissue expansion. The eyebrows tissues are firmly tight and making them drop down lower requires the creation of extra tissue to do so. Even in cases of custom brow bone augmentation you can not really make the eyebrows drop down significantly.
3) For your wide cheekbones you are referring to narrowing them which can be by standard cheekbone reduction surgery with anterior zygomatic body and posterior zygomatic arch osteotomies.
4) For wider hip bones you are referring to a procedure known as iliac crest reduction. (hip bone reduction) To learn more about that procedure I would refer to the following: www.exploreplasticsurgery.com and place in the search box the term, Iliac Crest Reduction.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I was wondering if you provide surgical and non surgical treatments to fix masseter muscle disinsertion. I had a custom jaw implant but the shape has come out round because of the muscle not filling the gonial. I heard Botox can be used and then guided to fill the gonial area. Have u had any experience with this and what would be the cost of you surgical treatment . Thank you
A: The cause of masseter muscle disinsertion (MMD) is either inadvertent separation of the psteryomasseteric sling during implant placement or an implant design that extends too far back beyond the muscle border. (which is an implant design issue and is better known as ‘implant reveal’. I do not understand the statement ‘ the shape has come out round because of the muscle not filling the gonial’ as the muscle is not what causes the implant shape at the angle.
In the treatment of true masseter muscle disinsertion (MMD)the fundamental options are to either 1) cover the exposed implant and 2) reduce the size of the muscle above it with Botox injections. (a short term but not a long term solution) #2 is a temporary non-surgical solution,. There is no such thing as ‘ I heard Botox can be used and then guided to fill the gonial area.‘ Botox is a muscle reducer not a soft tissue filling material.
In the surgical treatment of MMD them options are 1) muscle repositioning back over the implant, 2) fat injections over the implant, 3) alloderm grafts or synthetic soft tissue jaw angle implants. I have done them all and each of these methods has their distinct advantages and disadvantages.
Dr. EppleyDr. Barry Eppley
Indianapolis, Indiana