Your Questions
Your Questions
Q: Dr. Eppley, It is so hard to find a really good facial surgeon. I am 58 years old and in the past year 2 years my face fell! I lost 50 pounds, went through menopause and had way too much sun. My lower face is awful to me. My mental crease is over almost my whole chin and no one locally seems to know what could be done about it.
Any and all advice greatly appreciated.
I feel like my lower face is worse than most 80 year old faces I see? Sigh…the struggle is real.
Thank you for your time!
A: Thank you for your inquiry and sending your pictures. You have to throw out the chronology (age) and just look at the anatomic problem. For all of the reasons you have mentioned, particularly the weight loss, your degree of lax/falling tissues does not match your age. The foundational procedure is a full lower facelift which will make a world of difference. The central chin area, however, is not going to change no matter what is done laterally to it. I believe you are specifically referring to raised mounds under your lower lip but above the labiomental crease. These are subcutaneous fat collections for which microliposuction would be the only effective approach to reducing them. They are not that rare as they probably occur in 1% to 2% of the general population.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’m contacting you because I’ve had a complex about the shape of my skull for several years. Indeed, I find that my skull has the shape of an inverted “V” on the posterior saggital part. Consequently, as my hair is fine, flat and without volume, I have a hairstyle that looks like a “triangle” and this is not flattering. Also, when I tilt my head forward, the pointed side of my skull appears and the shape is not that of a harmonious rounding. When I tie my hair, I always pay attention to the elastic band to try to hide the defect of my head but often, the shape is still visible. I have added several photos as attachments so that you can see.
I have several questions if you agree to answer them:
First, I would like to know if you could suggest an aesthetic procedure to improve the shape of this part of my skull, to make it more rounded and harmonious, and if it would have a real aesthetic benefit for the overall beauty of my head (face + skull).
Would injections of my own fat be enough to improve the aesthetic aspect of my skull?
If not, should I consider a custom-made implant?
As I live in Europe, I would like to know if you have a colleague to recommend to me who works like you on cranial contouring.
Finally, could you give me a price range for such an operation?
Thank you in advance for your answer.
Best wishes,
A: Thank you for your inquiry, detailing your head shape concerns and sending your pictures. The definitive treatment for a scaphocephalic head shape is to either reduce the posterior sagittal crest (#1), bilateral parasagittal/temporal line augmentation (#2) or a combination of both. (#3) I will discard #1 and 3 for now and focus on #2 (volume addition) to which I can say the following:
1) While fat injections can be done anywhere, including the head, their volume retention in the tight scalp is precarious at best. But there is certainly no harm in doing so as a first attempt at skull augmentation. But the risk is high for either complete resorption or a minimal augmentation effect.
2) The definite and assured method of skull augmentation is a custom skull implant that is precisely made for your anatomy and aesthetic requirements. This is a common aesthetic skull augmentation procedure in my experience.
3) I am not aware of any European surgeons that perform this type of aesthetic skull reshaping surgery.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I was interested in facial implants. I’d like to know the cost of temple and cheek implants. I want a cheek implant that would give only projection and no width since I already have adequate width.
Also, would temple and cheek implant provide a subtle lift in the jaw area? I was considering a facelift but thought the face would look too tight after both the implants and the lift. I need very subtle lift in lower jaw area.
A: In answer to your facial implant questions:
1) To have cheek implants provide only forward projection and no width that may require a custom implant design. It would depend on knowing more about your specific midface augmentation goals.
2) Temple and cheek implants are not going to provide any lift in the jawline area as that is too distant from where the implants have any lifting effects …which is very modest in that regard anyway.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in skull augmentation. I can’t believe the amazing results you achieve. The shape of my head has bothered me for a long time. I have looked into having surgery here in the UK but my options were to have a very large cut and not like the small incisions you make. The results I would like the achieve are something very similar to the below image. I just have a few questions if possible? I was quoted in the UK with the large incision. Can the implants migrate? Can they cause headaches and can you feel the implants if you were to run your fingers through your hair?
A: In answer to your skull augmentation questions:
1) Onlay skull implants do not migrate regardless of their size.
2) Onlay skull implants have never caused headaches in my experience.
3) Onlay skull implants have a smooth contour and a seamelss edge transition onto the skull bone. Thus you can not feel them if you touch your head or run your fingers through your hair.
Dr. Barry Eppley
Indianapolis, Indiana
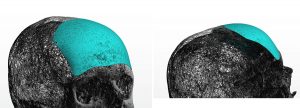
Q: Dr. Eppley, my goal is to reduce the head circumference in the back of the head with the goal to achieve a smaller head because in my opinion my head looks really big with 59 cm head circumference. I will link some pictures so you can see the problem I am talking about. The red marked in the picture is where I would like to reduce the skull size if possible. The ”bump” in the back of the skull so to speak.
And my last question, on an average for people like me who want to do this type of skull reduction in the back of the head, how much skull reduction is normal to expect less than 1 cm or a little bit more? Because I had a hard time finding answers online.
I just wanted to see what you would answer on these questions and after that I might book an online consultation.
Thank you for taking your time
A: In answer to your skull reduction questions:
1) I have imaged what I think is a realistic amount of back of the head skull reduction. As a general rule such skull reductions run in the range of 7mms of bone removed until the diploic space is reached…which is where one has to stop.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Dr. Eppley and his team seem top-notch – highly skilled and experienced. I would request for a consultation, but it is far, unfortunately. May I ask for expert advice and/or referral?
I have a recessed chin and no visible jawline which has bothered me since teenage years. Despite orthodontic treatment in the mid-90s (headgear + braces), my overbite persisted. I am embarrassed to say I still felt ugly, especially when I noticed my side profile in pictures at school. What’s worse, I did not use a retainer judiciously. Fast forward a couple decades and I have an appointment set for next week with a local orthodontist in Memphis, hoping to *finally* fix the overbite and some crowding that occurred over the last 8 years.
I have not seen the orthodontist yet, but I have been online reading a bit more, searching for doctors who have helped patients with similar profile photos as mine, looking at before+after photos. From these, I am reminded that braces alone will not help me with my lacking jawline + recessed chin. I discovered that I need help determining what would be the best approach: a chin implant, sliding genioplasty, or jaw surgery. Seeing that Dr. Eppley has helped so many patients with similar problems and facial features, would Dr. Eppley be able to determine which procedure would be needed? I attached photos of my face if that might help.
I have no jaw pain, my bite seems okay other than the overbite. My face is slightly asymmetric (left cheek? larger than right). Simply put, I don’t think I need jaw surgery but I am unsure. If I only need a chin implant, that’s a relief, but if I need a sliding genioplasty, could I possibly find a surgeon with similar expertise as Dr. Eppley?
Thank you for taking the time to consider my case (photos attached)!
A: Thank you for your inquiry and sending your pictures. Like all chin augmentation patients one always has the option of a chin implant vs sliding genioplasty. While I think you would be best served by the sliding genioplasty long term, there is nothing wrong with a chin implant option…as long as it is the right chin implant style for a female and it is securely positioned on the bone.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had 9 months ago a ZSO (zygomatic sandwich osteotomy) procedure. I don’t like the outcome. My surgeon used bone marrow from my hip. Is it possible to revise this procedure? Do I assume right, that you would just pull the graft material ( in this case bone marrow) out and push my cheek bones together again?
Is the revision more risky than the former procedure?
A: You can reverse a ZSO (zygomatic sandwich osteotomy) by a wedge resection of the now healed grafted bone and putting it back where it originally was. It has no more risk than the original procedure minus the need for a painful donor site.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, thank you or your understanding and expertise, but I value my frontal face angle more than my side so I don’t mind altering the profile. Like I said I wanted to reduce my cheek size when I smile but you explained that wasn’t possible. How about the soft tissue bulges at the side of my nose when static (as seen in the pictures), can they be fixed with cheek implants/paranasal as I desire a more robust frontal look like the model? Can the cheek implant alone stretch that area so that light hits the malar area instead of my midface or will paranasal be required too. Finally can implants in my face cause my cheeks to pop out more when I smile? If this is possible then I would like to schedule a consultation to discuss more about this.
Thank you
A: While paranasal/midface implants can push the tissues forward along the side of the nose I can not say whether that would be enough to flatten the bulges to which you refer. In theory it should…but that remains an as yet unproven theory in your case.
Whether cheek implants can stretch the soft tissues to change the soft tissue highlights would be heavily dependent on their shape and size. That is another one where that should be possible but not completely predictable.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’m a body builder who wants some help getting a classic v-taper to my body. I think the hip bone shaving procedure is what I’ve been looking for. But how much volume does this actually remove from the hip area?
Thank you so much!
A: On average the widest part of the iliac crest that can be reduced (hip bone shaving) is in the 1 to 1.5cms range. But for a very active person (aka body builder) this would not bs the type of patient I would be comfortable performing such surgery in because how it may effect the ability to quickly get back to that physical activity and the always unknown issue of potentially chronic discomfort with that very active lifestyle.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’m wondering the cost for a nostril reduction/ Alarplasty. I’m not looking to make any changes to my tip or bridge, I’d just like smaller nostrils.
A: Thank you for your inquiry and sending your pictures. The wide flare of your nostrils requires a combined width and height reduction of them which means that a wedge of the nostril is removed. This places a scar line from inside the nostril and around the sides of the alar-facial groove. Whie these scars general do well there is always the chance of some scar visibility particularly when more natural pigment exists in the skin. Thus it is always better to think of this more aggressive form of nostril reduction/narrowing as a two stage procedure with the hope that the second stage (scar revision) is never needed.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hi! I am transgender, and like many trans women I struggle with feminizing the lower half of my body. I am ectomorpbic body type and would like to maintain a supermodel structure, but I am struggling with my bodies proportions. This may seem strange but I am wondering if there can be customized implants for the iliac crest of the pelvic bone so that it gives me the appearance of a wider and more feminine pelvic bone? I see a lot of hip and butt implants, but I am wanting something that will feminize my body in a skeletal, anatomical way. Thank you.
A: Thank you for your inquiry on what is known as iliac crest implants which would create a wider pelvic bone. That is as concept that I have been working on for the very need to which you speak. This is really a cap applied to the widest part of the rim of the iliac crest. While one could argue it should ideally be made of metal, I have found no orthopedic manufacturer in the U.S. willing do so I am looking at an ultrafirm solid silicone material for the iliac crest implant.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I was just wondering if it would be at all possible to design two testicular implants that would have a total size of 120 cc’s that could be implanted over existing testicles?
A:That is too high a volume if you are speaking of 120ccs per side. If you mean 60ccs per side then that is possible to do.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had a double chin, recessed chin and no jawline, so I got a chin implant, buccal fat removal (sank one side of my face, I hate it), and now my chin looks too wide and longer. My neck is short and I feel it doesn’t suit my face shape or posture.
I would like a v-shaped chin, but much like my own (since I always felt pretty except in my late 30’s my neck started melting).
The other doctor helped my jawline look at bit better, he said I didn’t need a necklift.
The doctor said a genioplasty won’t stretch my lower face too much. I want to age nicely in my neck, since my family are fat faces, necks, no jaw.
I don’t know what is the best shape for me. Please help! What do you suggest?
A: Thank you for your inquiry and sending your pictures. I am little unclear as to exactly what you are trying to achieve. You have the classic female chin problem where the implant used is too wide due to having wings and is probably positioned too low on the bone…hence making your chin wider and longer. But in trying to get a chin that is horizontally shorter (which I assume is what your natural chin is) that is also more narrow/v-shaped is going to be a problem. Implant removal is going to cause an excessive/lax soft tissue chin pad because it has been stretched out from the implant and will not magically shrink back down.
This leaves you with three options:
1) Get a new chin implant that is v-shaped and sits higher on the bone and live with the exiting horizontal projection,
2) Remove the existing chin implant and replace it with a t-shaped sliding genioplasty, or
3) Through a submental approach remove the existing chin implant and shave down the sides of the chin to a v-shape and tighten the soft tissue chin pad by a submental tuck.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have a wide zygoma arch, and I’ve considering a cheekbone reduction for some time. But I’ve not read review of a single person anywhere who was happy with it. In fact I ran into many people who warn against the cheekbone reduction surgery as it causes droopy eyes and sagging skin. People end up getting face lifts and implants after it. I am attaching an image that will give you an idea of what I look like, however the result of the girl after the surgery doesn’t look great, I’m not sure for what reason. It looks bit extreme. I want to reduce just the width at the back, dont want to reduce the prominence of the cheekbone. I hope you’ll be able to provide me some insight, I have read so much on forums and all and can’t seem to understand as to why the result of this surgery are almost never satisfactory. Both my temples and jaw look concave because of my wide zygoma arch. Will the skin be saggy and eyes droopy due to lack of support and overall lack of definition even if I seek to reduce only 4mm or less at back of the cheekbone (only the arch)?
Having done some surgeries already in the past I don’t want to take up a huge risk again, kindly refer to the pic attached and let me know if it will be worth it or not. I appreciate your help, thank you so much.
A: I certainly can not tell you whether you should or should not do cheekbone reduction surgery. All I can do is provide you with my experience with the procedure.
1) It is not my experience that the vast majority of cheekbone reduction surgery patients are unhappy or require secomdary management surgery. There are many satisfied patients from cheekbone reduction surgery but they less frequently are the ones most vocal on the internet. But like all aesthetic surgeries there are risks and tradeoffs. The risks are cheek asymmetries and over/under correction. The tradeoffs are potential soft tissue sagging, often of a relatively minor degree since most patients who undergo the surgery are young with better quality tissues.
2) There are many technical variations of cheekbone reduction surgery but the most important of them is the amount of inward bony movement that is done. It can be from 1mm to 10mms. The amount of inward movement is going to affect the risk of soft tissue sagging…the more inward movement the more likely some soft tissue sag will appear after surgery. Many times this operation is done maximally (in a cookie cutter fashion) and those are the patients most likely to experience postop soft tissue sag. The reality of these statements is that the patient has to make an informed choice before surgety….how aggressive does one want the cheekbone reduction to be vs what risk is one willing to take in altering one’s natural facial bone structure onto which the soft tissues are made to be. For some patients it is often better to compromise…accept some but perhaps not ideal reduction to mitigate the postoperative risks.
3) In aesthetic surgery there is always a completely assured way to avoid the risks…don’t do the surgery. After all this is purely elective and your life will continue onward without doing the surgery. As a general observation patients that have deep seated fears about surgical risks are not good candidates for surgery.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Would a brow implant result in a lower and more straight brow ridge? Or does it simply enlarge the brow ridge.
A: Because it is a custom design the brow bone implant can be made to have any shape one wants.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had a couple specific questions regarding custom silicone midface implants (covering the front part of the zygoma as well as the arch up to the temporal bone and the infra orbital rim) and genioplasty
1.) Would there be any issue on your end with performing the implants on a patient who has had MSE in the past? (maxillary skeletal expander). I ask because the way in which the bizygomatic width increases after this procedure (multiple studies confirm it does) is still unclear to me. If the frontozygomatic sutures are loosened I can imagine some sort of extra width possible without compromising the height or at least the perceived height of the cheekbone. Otherwise, if its fully from a sort of rotation where the arches are angled outward, wouldnt the cheekbones appear lower set post op since the area of the zygomatic arch that protrudes laterally the most would now be lower than pre mse? If this is the case, could you place implants to make the upper-most part of the arch the widest again and resolve this? Would getting both mse and custom implants on the zygomatic arches be redundant then, strictly from an aesthetic vantage point (as opposed to sarpe in lieu of mse and then implants at a later date)?
2.) Can a genioplasty be performed such so that the chin travels along the occlusal plane, eliminating unsightly step off points and increasing vertical height as well as anterior projection ?? (I imagine if such a thing is done, the chin is simply mobilized and fully removed from the mandible and re positioned, then new bone fills in or if the movement was large enough to necessitate this, a graft is used as a buttress).
Thank you very much for the help and Id like to extend my thanks for the entirety of your blog, its very helpful to be able to read succinct snippets of your insight and send inquires to such an authority within the field in a colloquial manner.
A: In answer to your questions:
1) Regardless of what type of maxillary expansion you may have had your frontozygomatic sutures are not ‘loose’ or have been loosed in so doing. Any discussion about your facial skeletal form at any level can not be done on an informed basis without the knowledge of your bony anatomy from a 3D CT scan.
2) While the chin bone can be moved in any direction some bony irregularities along the inferior border and in the convex shape of the anterior chin surface are inevitable. The magnitude of them depends of type of chin movements done.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, For years I’ve been bothered by the feeling of having some form of excess tissue inside my cheeks at the sides of my mouth. I’ve tried naturally losing weight, ultrasound skin tightening therapy, visiting an oral surgeon and investigating buccal fat pad removal, but all have either had no effect or have told me there’s nothing they can do.
Given how much this bothers me (I find myself sucking on the tissue 24/7 trying to get it out of the way of my mouth), I’m desperate to find some resolution.
I came across your site and read about Perioral mounds, and it seems as though this best fits my problem. I’ve attached some images highlighting the problem area, and was wondering whether I’d be a candidate for Perioral Mound micro-liposuction?
Thanks in advance
A: You have redundant mucosa in the inside of your cheeks which can be removed by a horizontal elliptical excision. (intraoral cheek reduction) While this will remove the intraoral issues that will probably not provide much improvement to the external appearance which is more consistent with perioral subcutaneous fat collections.
Dr. Barry Eppley
Indianapolis, Indiana
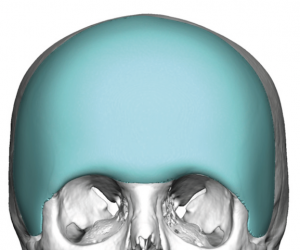
Q: Dr. Eppley, Procedure (s) recommended for making forehead larger, wider, rounder, more contour and lifting volume in glandular region and above brows- more feminine look and less convex face.
A: Thank you for your inquiry and sending all of your pictures. Your facial upper third enhancement goals, which is a not uncommon request for females, can only be achieved by some version of a custom forehead or forehead-temporal implant. It just depends on how extensive in surface areas coverage the augmentative effect needs to be.
 A conservative or limited forehead augmentation effect can be achieved with a design that extends not further than the bony temporal line of the sides of the forehead. (see attached)
A conservative or limited forehead augmentation effect can be achieved with a design that extends not further than the bony temporal line of the sides of the forehead. (see attached)
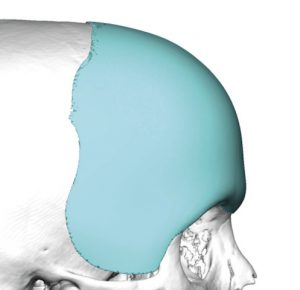 Or a more complete forehead-temporal augmentation can be done by a design that crosses well over the bony temporal line which is appropriate for those women that have a natural flatter and narrow forehead shape. (see attached)
Or a more complete forehead-temporal augmentation can be done by a design that crosses well over the bony temporal line which is appropriate for those women that have a natural flatter and narrow forehead shape. (see attached)
And there are numerous variations between these two ends of the custom forehead implant styles.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hello I read the article about how a custom jaw and skull implant is highly unlikely to fracture or dislocate due to how much surface they take up. My question is regarding the custom cheekbone implants. Will there be a higher risk of fracture or dislocation. I am a male in mid 20´s that trains in boxing recreationally.
A: When I speak of fracture or dislocation in regards to facial implants, and custom facial implants in particular, I am referring to the bone underneath them. Given the coverage of the bone by the implant, which virtually acts like a bumper on the bone, it would make bone injury underneath it much less likely due to the implant’s shock-absorbing and force redistribution effect.
I am assuming you are not referring to the actual implant being fractured (which is virtually impossible) or being displaced. (also very unlikely)
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hi! I had some questions about hip augmentation with implants, as well as thigh implants to give the thighs more of a “chubbier” look since I personally think thicker legs are pretty.
1st, would it be possible to make hip implants that could be put on the bones/under the muscle in the legs/pelvis to make them feel as natural as possible?
2nd, is it even possible to make thigh implants that would make the legs look a bit wider at the sides of the thighs? I’ll insert a picture of the kind of legs I mean. Instead of making them look toned or defined just kind of making them look less skinny and more soft.
A: In answer to your hip and thigh implant questions:
1) Hip implants can not be placed under the muscle or next to the bone.
2) Thigh implant can be placed more laterally under the TFL for a more lateral/wider thigh look.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have a couple questions about the posterior zygomatic arch osteotomy I forgot to ask during my virtual consultation I was hoping you could answer for me:
1) Will I have a tough time eating post surgery? I’m not sure if working on the zygoma influences the masseter muscle at all and if this will lead to pain during jaw opening and closing for the first several days?
2) With the posterior arch osteotomy and plate fixation, Can Dr. Eppley plate the arch onto the skull a bit higher than where it was originally? In order to bring the entire arch higher and make my cheekbones higher?
A: In answer to posterior zygomatic arch osteotomy questions:
1) The posterior zygomatic arch osteotomy will not affect the masseter muscle or eating in any manner. The masseter muscle attachments are more anterior along the zygomatic arch.
2) The zygomatic arch can not be moved/relocated higher. And even if the posterior end of the arch could be moved higher it would not create the high cheekbone look.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’m fairly sure I have nasomaxillary hypoplasia (not to be confused with Couzon’s Syndrome-tier midfacial hypoplasia). The whole area around my nose (zygomas, maxilla, infraorbitals) is recessed and this not only puts me at a great aesthetic disadvantage but also causes me severe obstructive sleep apnea that’s refractory to traditional treatments (mouthpiece, CPAP machine, weightloss – I’m not currently obese).
As such, I need a Lefort 2 Osteotomy.
My question to you is: In an effort to minimize the risk of death during the surgery (if I recall correctly, the LF2 osteotomy is supposed to have a 10% mortality rate but I might be confusing it with the LF3 osteotomy), is it surgically possible to completely leave out the nasal bones and only move forward and/or lift the remaining portion of the midface, ie.: zygomas, infraorbitals and maxilla?
Below, I’m attaching the relevant picture(s) of my face showcasing my nasomaxillary hypoplasia. (the text says: the maxilla, the zygomas and the infraorbital bones are severely recessed. the philtrum appears to be long and flat)
Thank you in advance!
A: I am not aware of any risk of death from any form of Lefort osteotomies regardless of the level at which it is done.
What you are describing is what is commonly known as a modified LeFort III osteotomy.
Dr. Barry Eppley
Indianaplis, Indiana
Q: Dr. Eppley, I have provided a picture of an example of the pectoral gap I am talking about. Would it be possible to make the pecs appear closer together? For instance, perhaps putting an implant on the inside part of each pec to make the gap smaller? Would this be possible? Thanks.
A: Thank you for sending your picture. I believe you are referring to placing an implant under the pec major muscle to add volume…which is all that can be done practically but with these caveats:
1) The sternal border of the pectorals major muscle will get bigger/have more volume but will not necessarily move the medial muscle border further into the sternal valley.
2) Such a pectoral implant can not just be a limited implant that only covers the medial area of the muscle as it will be unstable and will slide away from it. It must be an implant that covers the entire subpectoral pocket to be stable. It can have its greatest volume along the medial muscle border but it must have a footprint that covers the whole subpectoral space.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am a 26 year old petite female with narrow shoulders. I would like to add 3-5 cm on each shoulder. Is shoulder augmentation via silicone implants an option for me? Or will it make me look masculine/bulky?
A: Shoulder augmentation by deltoid implants is going to add 1 to 1,5cms per side in a petite female. An increase of 3 to 5 cms, even if it were possible, would look out of place and bulky on all females and even in most males.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in doing shoulder widening and I have some questions regarding that:
1) Regarding deltoid implant: if it is placed over muscles, and if a person works out, wouldn’t implant somehow be in a way of muscle growth? what I mean is if the muscle can grow a lot via weight training, wouldn’t the implant hinder that?
2) If it is placed over muscle, how is the implant fixated?
A: In answer to your shoulder widening by deltoid implant questions:
1) Subfascial deltoid implants sit on top of the muscle so they would be pushed out with the muscle should it develop hypertrophy. It would not induce a hindrance on muscle growth.
2) Like all subfascial muscle implants it is the scar encapsulation which provides all the fixation that it needs.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in doing shoulder widening and I have some questions regarding that:
Can you do multiple clavicle lenthening procedures? – let’s say that 4 cm per side increase would be perfect for me but as you answered in another question, increase of 2 cm per side is maximum, because of fear of bone not healing properly. Could I possibly do one clavicle lengthening surgery now and another on after year or two.
A: In answer to your shoulder widening by clavicular lengthening questions:
I have never done a two stage clavicle lengthening procedure so I can not speak as to its viability. I would say that if the initial clavicle lengthening procedure healed satisfactorily I would not tempt fate and do it again a second time.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have asked about having a submental approach to fixing a hyperdynamic chin ptosis. You have advised against having this surgery due to the fact my chin will slightly decrease, and of course, I want to preserve my chin appearance at rest.
However I have a oral and maxillofacial surgeon that only works on facial surgery and says he will only works on the mentalis muscle and preserves my chin at rest. I need to know if this is possible, as I don’t want to spend so much money on fixing something that may worsen.
A very slight decrease is fine by me, but not in a way that will make my chin look recessed in any way.
He said it is not my chin that needs fixing, it is the mentalis muscle. I’m wondering how does one suspend the mentalis muscle Without the chin being affected. Is this possible? have you done this before yourself?
My chin at rest is not protruding in any way or big.
Please can you help me with this?
A: I do not comment on other surgeon’s technique or whether what they say they can do is possible or not.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Growing up I’ve always had dark circles and deep hollows under my eyes due to hereditary reasons. So around two years ago I tried filler for the first time and unfortunately it created a darker tint. Looking forward, I was hoping to find a more accurate and permanent solution to the issue. I then learned about the orbital rim implants from your page and was fascinated by your work! Reading about the orbital rim implants from your page I appreciate how the implant covers the tear trough deformity and rings simultaneously, which were my main concerns. Also reading, I saw that the results could also be adjustable if any inconvenience which really got me on board. I was initially concerned regarding scleral show, but then read that typically it must be done with a well done canthopexy to maintain and avoid the problem worsening. I attached some photos below and would love to hear back from you soon! I greatly appreciate your time Dr. Eppley. Thank you.
A: Thank you for your inquiry and sending all of your pictures. You are correct in that custom infraorbital-malar implants are the preferred correction for your undereye concerns. You are also correct in that lower eyelid management is important during the closure. While you did not show a side view picture, it is likely you have a negative orbital vector.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, My forehead has a weird shape to it. I’ve had two bumps (horns) on it for as long as I can remember. I would like them removed if possible. My concern is that my hairline is receding badly, so I’m unsure if I’m even a candidate to have the procedure done. I know that affects the placement of the incision(s). How much does the procedure cost. Please inform me of what you think. Thanks for your time.
A: Thank you for your inquiry and sending your forehead picture. While such forehead horns can be successfully removed the challenge is the incisional access to do so. With your hairline being so far behind the front of the forehead it can not be used for access to perform the procedure. While incision further forward can be used for access my concern would be that you would just be trading off one aesthetic problem for another. (forehead horns fora visible scar)
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Are there any procedures that would allow trans man’s hips to become more narrow? I read about iliac crest reduction but I was wondering if there other possible procedures that could make a bigger difference. Is there such a thing as cutting through a specific section of the upper ilium and tilting it closer to the belly button (I hope that doesn’t sound ridiculous)? I understand that even if such a thing did exist it would be high risk, but it’s definitely something I would be interested in.
A: The answer is that there are no other hip narrowing procedures. Trying to cut and move/tilt the pelvic bone is an interesting mechanical drawing concept but not a practical one in terms of medical safety and complication risks.
Dr. Barry Eppley
Indianapolis, Indiana